

To wrap up our section on lumbar disc injury, Nina and I break down some of the most common patient questions we receive. As an AT, Nina is accustom to triaging athletes in pain, helping them find confidence in their plan of care.
SV: For the past month, we’ve been sharing the latest research on lumbar disc pathologies. As a recap, what are your top three take aways for experiencing back pain?
NS: We’ve covered a ton of information on this topic recently, looking at the impact of pregnancy as well as injury. The overall takeaway is that each individual’s experience can be different- this goes for symptoms and solutions. That’s why personalized care can have such a big impact for back pain. Similarly, there isn’t one guaranteed strategy for managing a lumbar disc injury. A combination of treatments, including soft tissue work, stability and mobility exercises, and pain management, is typically needed. Last, use this as an opportunity. For most people, an injury like a disc herniation can be a catalyst to make adjustments to their behaviors, allowing them to emerge stronger than before.
SV: How does this differ from the type of back pain caused by pulling a muscle?
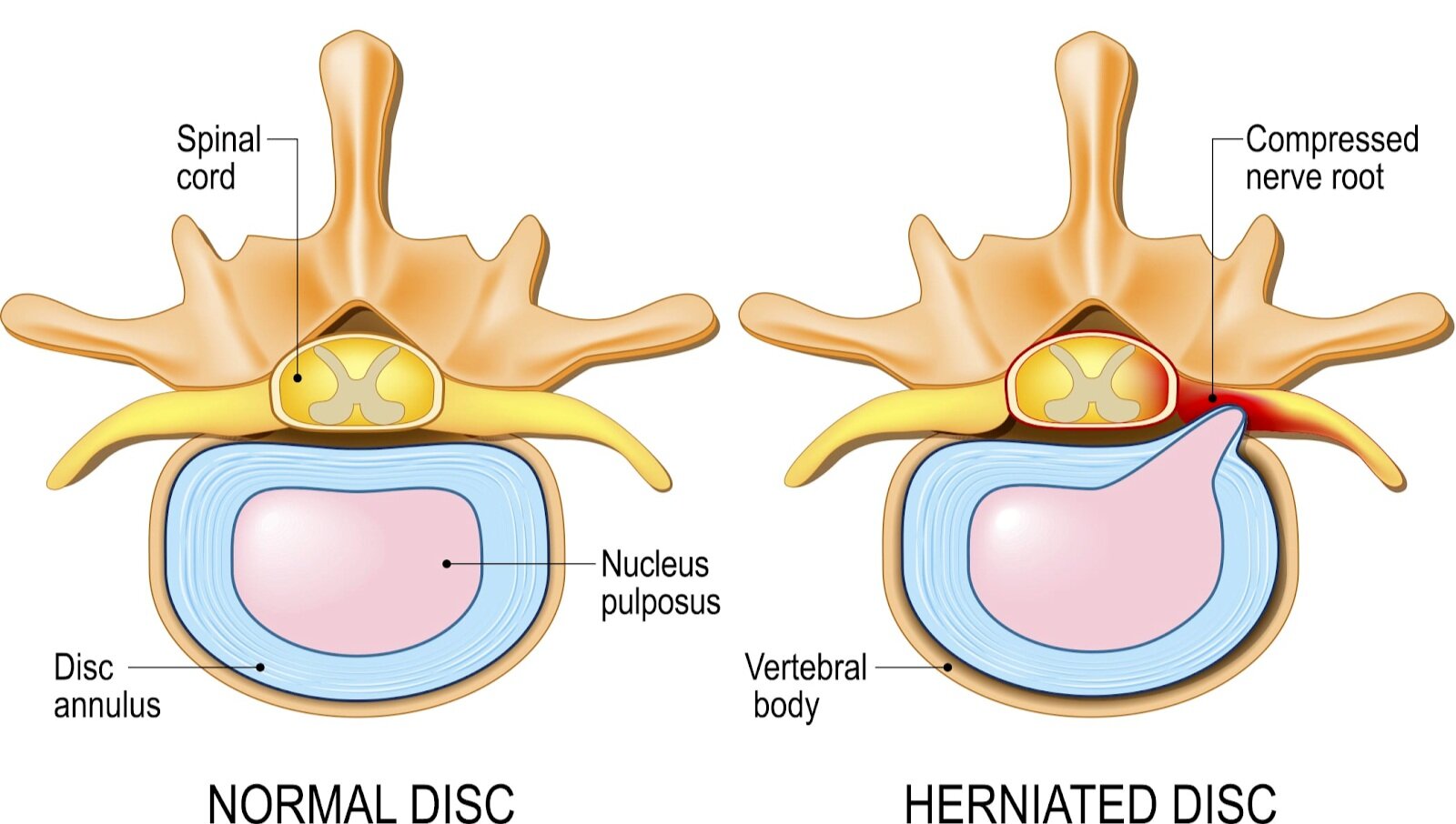
NS: Discogenic pain has a different quality; many patients report feeling sharp, electric sensations, while others complain of weakness. Nerve pain can “travel,” sending irritation down one or both legs. Muscle spasm often accompanies a disc injury- it’s a protective strategy. Muscles of the back will automatically tighten above and below the injured disc to limit movement. This tightening makes it difficult to use muscle systems, or groups of muscles designed to support compound movements, effectively.
Pulling a muscle, or overusing a muscle, can usually be correlated with a specific action or activity. You may feel tight, or restricted. This should resolve, or feel considerably better, in 72 hours if it’s just muscular.
SV: Here’s a popular combo question- do patients need to get imaging for this type of injury? How likely will they need surgery?
NS: It’s a valid question- too often, we only hear about worst case scenarios for injuries. Unless you’ve suffered a traumatic injury, like a car crash, we don’t typically recommend imaging right away. Rehab exercises and pain management will be the most productive first steps. If you eventually need surgery down the road, being as strong as possible going in will dramatically help your recovery!
Surgery makes the most sense for patients who have a high risk of complications- like if your herniation or displacement is so severe you may cause permanent damage to your spinal column- or for those who haven’t succeeded with conservative care after a number of months.
We’re big believers that patients should be the center of their plan of care, with a variety of clinicians and specialists, coaches and supporters surrounding them. Without a different perspectives, you can overlook options. Ask questions, get second options- be your best advocate!
SV: Once someone injures their back, does that mean they can never workout or play sports again?
NS: In the vast majority of cases, definitely not! Most patients are able to return fully to their previous level of activity. Like any major injury, it will take dedication and focus to recover. It’s essential to allow your body enough time to heal, and to correctly learn, or re-learn, movement patterns. Look for rehab practitioners that understand the demands of your activity, and can help get you there. Stopping at 65-75% better increases your chance of re-injury significantly.
SV: With back pain being one of the most prevalent injuries, how can someone lower their risk for injury?
NS: Regular physical activity will help to protect against a number of ailments and injuries. Particularly with the recent transition to virtual learning and working, movement is even more important, as we are naturally more sedentary in this scenario. Adding in tri-planar exercise, including linear, lateral and rotational work, can help make sure you’re prepared for whatever life throws you! If you’re new to exercise, or struggling with home exercise routines, setting up an appointment to work with a clinician or coach can give you the confidence you need to move safely.
SV: At Physical TheraPT, as many of our patients know, we love staying current on the latest innovations in exercise and rehab equipment. What’s your favorite product out there right now for back pain patients?
NS: For patients still in the early stages of recovery, I really like the biofeedback cuff. This deconstructed blood pressure cuff helps increase awareness of pelvic stability and highlights how well someone is able to maintain a braced position when you add on movement. For those who are out of pain, and show progress with more challenging exercises, the 3D strap is my favorite. Don’t be deceived by the simple nature of this piece of equipment! It adds rotational load to almost any movement pattern, allowing athletes to adapt and practice in a safe environment.


SV: Last question- what’s your go-to strategy for pain relief with this type of injury?
NS: Finding a position of comfort that you can rest in. Back injuries can feel unrelenting- having a position that gives you some relief is critical in the beginning stages of recovery. Laying on a firm surface, resting on your back with knees bent and feet planted, referred to as Hook-Lying Position, is generally safe for most patients. Others may find relief with a bit of light traction, leaning into your elbows at a counter, or floating in a pool.